

- Seasons
- Summer
- Healing
- Autumn / Fall
- Spring
- How I view Forgiveness
- Winter
- Loss of a child
- Ideas for Self Care
- On the arrival of Illness
- Soul Doubt
- Life & Death
- Wanting Memories
- Covid Questions to be considered
These are a few of the questions that you may have been asking yourself about the way the Covid-19 virus has been handled by world governments.
1 We now know that several Nations (USA, Canada, China, UK) were financially involved in the Wuhan labs that created the covid-19 virus.What were their intentions with such research?
Why won’t they tell us? What are they hiding?
Why are they pushing inadequately tested vaccines when these are not only causing death and morbidity, but may not be providing overall benefit?
2 Does this involvement explain the participant Nations’ governments as leaders in a cooperative effort? Is it not suspicious that for the first time in the world : many world governments agreed to promote international lockdowns within months of ‘discovering’ covid-19?
3 Given the inaccuracy of covid tests and reporting {c.f. Evidence point 1 below}, to determine the pandemic effects surely we can at least rely on mortality (death) rates?. This is claimed to be nearly 5 million deaths since the release of covid to August 2021. However many/all countries statistics attributed any death with covid a covid positive death to be a covid death.The majority of “covid deaths” (over 90%) have been either people over 80 and / or with significant co-morbidities. In other words they could have died from natural causes or from existing disease.
Why is the low risk of covid to healthy people under 80 not promoted?Has there been a statistical reduction for those deaths in order to look at the actual effect of covid on the healthier/younger population, and then weighing that against the deaths from suicide, violence and lost medical opportunity?
4 By taking out this 90% bias we are left with a global mortality (death count) for covid which is somewhere around 500 thousand deaths world wide.This is to be compared with the WHO reporting of annual deaths such as:
- world wide car accidents (1.3 million),
- Normal flu worldwide (290- 600k)
- Kidney failure (1 million)
- Abortion from fear or poverty (100 million +)
Yet a great part of the world was locked down and suffered isolation and constraint for a virus that was man made?Why?How can this be called a pandemic if the flu is not a pandemic?
5 There have been trillions spent on covid remediation and vaccines. If that amount were applied to other causes of death and suffering?e.g. War and conflict 500KSuicide 1.5 Millionstarvation worldwide up to 9 million lives
Why is starvation not even counted in the top 10 causes of death?Could it be because starvation primarily happens in areas that are not wealthy?Hence why when you look at the map of where covid vaccines are distributed you will find it is almost all in wealthy countries. Only 25 % of the world is vaccinated and yet the media is pushing that vaccines will lead to no lockdowns, when those countries that are almost fully vaccinated (e.g. UK, Israel) are not showing any significant change in rates, because the covid deaths in vaccinated individuals (called ‘breakouts’) is on a par with unvaccinated.
6 The role of BIG Pharma in vaccines.Did you know that 75% of the FDA’s funding is provided by big Pharma?
Some big pharmaceutical companies have used illegal methods to justify dangerous drugs in the past, and that includes modifying or purchasing false evidence to show safety. They have negotiated no legal comeback with the covid vaccines which are experimental and have caused millions of adverse events and at least 20,000 deaths and similar numbers of permanent disablements.
Why is it that other drugs are withdrawn from use after one or two deaths, and yet these Covid vaccines with tens of thousands of deaths are still being allowed to be administered?Are big Pharma being protected or able to buy government support for unsafe vaccines?
7 the role of the media.The media is feeding off the fear, it makes money from bad news.
Should governments be providing formal information regarding the true facts about covid, and trying to stamp down on fear mongering?
EVIDENCE to consider
1 Incorrect PCR results about a third of swab tests are done in those with clinical needs or in health-care workers. At the end of July, 2020, the positivity rate of swab tests within this group was (1·7%)
The current rate of operational false-positive swab tests in the UK is unknown; preliminary estimates show it could be somewhere between 0·8% and 4·0%.2, 6 This rate could translate into a significant proportion of false-positive results daily due to the current low prevalence of the virus in the UK population, adversely affecting the positive predictive value of the test.2
TRANSLATION:If 1000 people are tested using the ‘gold standard’ PCR test then at the time of this study 1.7% or 17 people were found positive.HOWEVER of that 1000 people the false positives were somewhere between 8 and 40.This means that the actual number testing positive could have been between 0-9 – {ie in the range 0-0.09%} so low (less than flu rates) that gloom and doom statistics based on the PCR tests are unreliable, yet are still used as the major predictor of trends.(Note the hyperlinks refer to the study details)
Studies of false-negative (FN) results from respiratory samples for SARS-CoV-2 are variable demonstrating FN rates (FNRs) ranging from 1 to 30% [1, 2]. FN results can occur for numerous reasons including suboptimal specimen collection, testing too early in the disease process, low analytic sensitivity, inappropriate specimen type, low viral load, or variability in viral shedding [3,4,5,6,7,8,9].
TRANSLATION:of the 1000 who were tested, 10 to 300 could have been falsely negative. In other words up to 300 people may have to be tested again and again, in order to establish if they could be positive… and if they do show positive, remember that 0-.009% of those may indeed be negative.
2 Mask Usage does not stop transmission, and its effectiveness is unproven
The virus that causes COVID-19 is about 0.1 micrometer in diameter. (A micrometer (µm) is one one-thousandth of a millimeter.) The holes in woven cloth are visible to the naked eye and may be five to 200 micrometers in diameter.
The word “droplet” means a coarse particle five micrometers or larger, while “aerosol” is the fine particles smaller than five micrometers in effective diameter. While Covid may be in a droplet, and a mask can trap some droplets, the actual Covid virus is so small that if air can get through, then it can too!
As to the extent of which you need the virus to enter your lungs in order to acquire a Covid infection, a single virus can settle and replicate, depending upon your natural (or acquired) immunity.
Masks cannot and do not stop viral infection. They MAY reduce some of the viral load (viruses contained in droplets may for example be filtered out) but if there is a viral carrier in an enclosed room, it is likely some of the virus will be passed onto you, mask or not.
This is why mask usage has been debated, argued over and recommended by the WHO, then withdrawn, as in many countries and provinces.
The raw fact is that it MAY be more dangerous to wear a mask than to not wear one, especially if the mask has already been used in an enclosed space with a viral carrier, and hence may have the virus resident in the fibers. As a virus can be trapped in a fiber, so also it can be released from a fiber, and continue on its journey at a later date. It is not a living thing.
Despite the lack of quantitative evidence, many countries have included recommendations in their pandemic plans on the use of face masks (16–18).
from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2662657/
see also https://science.sciencemag.org/content/372/6549/1439
In November, researchers at Bond University in Australia reviewed the results of 67 papers that considered mask wearing.
Two of the review’s authors said in a summary of their findings: “We know masks are effective in laboratory studies, and we know they are effective as part of personal protective equipment for health care workers. But that effect appears diminished in community usage.”
They explained “Urgent research is also needed on methods and designs to mitigate the downsides of face mask wearing, particularly the assessment of possible alternatives “
https://pure.bond.edu.au/ws/portalfiles/portal/63972883/Downsides_of_face_masks_and_possible.pdf
A Danish study of 6000 people late 2020 showed that “mask wearing showed no statistical difference to not wearing a mask” was then criticised by mask advocates, but no recent research papers have been published – why has this not been a world priority, or if they are available are the results just being held back because it would be too embarrassing? “Several trials have evaluated the impact on respiratory infections by use of surgical and N95 masks, which may, at best, modestly reduce acute respiratory infection transmission.” April 2021 reference to a study of papers on the subject Cowling BJ, Fung ROP, Cheng CKY, et al. Preliminary findings of a randomized trial of non-pharmaceutical interventions to prevent influenza transmission in households. PLoS One 2008;3:e2101.





 congregation. However the death of both her mother and her daughter led her to look for a different level of connection to what she gained from her weekend religious activities. Through LISN membership Annabel found inspiration from others who have had similar losses, and who were nearby.
congregation. However the death of both her mother and her daughter led her to look for a different level of connection to what she gained from her weekend religious activities. Through LISN membership Annabel found inspiration from others who have had similar losses, and who were nearby. Ethelia is lonely, new to her new village, and with specific spiritual interests which could be called ‘mystic’. Her country does not permit views contrary to the national religion. Ethelia longs for people to explore questions and inspiration with, and finds LISN.
Ethelia is lonely, new to her new village, and with specific spiritual interests which could be called ‘mystic’. Her country does not permit views contrary to the national religion. Ethelia longs for people to explore questions and inspiration with, and finds LISN. anyone else knowing what they are. He likes that.
anyone else knowing what they are. He likes that. He joined LISN and then discovered he can also upload his entire cohort of parishioners as users, so that they are part of the membership of LISN, but specifically assigned to his care group.
He joined LISN and then discovered he can also upload his entire cohort of parishioners as users, so that they are part of the membership of LISN, but specifically assigned to his care group. He had recently found a number of small groups existed that he did not know about. His attempts to get people to let him know had not worked, probably because things were constantly changing and there was no online method for people to update their own connections.
He had recently found a number of small groups existed that he did not know about. His attempts to get people to let him know had not worked, probably because things were constantly changing and there was no online method for people to update their own connections. She looked online and found lots of offerings but no indication if they would match what she was looking for. By registering and defining membership with LISN she was able to define her own spiritual expectations in a fun way, and in doing so the list of local Spiritual Directors was somehow narrowed down to those who matched her needs and style. She loved not having to research a whole lot of options and found it easy to choose one that works well with her spirit.
She looked online and found lots of offerings but no indication if they would match what she was looking for. By registering and defining membership with LISN she was able to define her own spiritual expectations in a fun way, and in doing so the list of local Spiritual Directors was somehow narrowed down to those who matched her needs and style. She loved not having to research a whole lot of options and found it easy to choose one that works well with her spirit.
 becomes:
becomes:





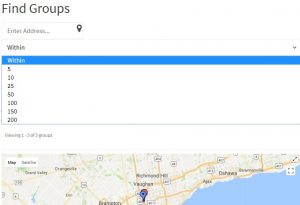
 LISN also has mapping and organizational support for small groups, circles, councils. LISN can link a person to spiritual circles or groups who are local or in a vicinity of interest.
LISN also has mapping and organizational support for small groups, circles, councils. LISN can link a person to spiritual circles or groups who are local or in a vicinity of interest.


 The content of LISN is kept in pages of information, which are categorized according to content. You can find such pages filtered by category, by selecting the LISN category from the side bar drop-down list. You can find Interactive Question Surveys (IQS) is a category.
The content of LISN is kept in pages of information, which are categorized according to content. You can find such pages filtered by category, by selecting the LISN category from the side bar drop-down list. You can find Interactive Question Surveys (IQS) is a category.
 Click here to go to the glossary and learn more.
Click here to go to the glossary and learn more.

 or enter your search address for where you are.
or enter your search address for where you are.














{kind=link}
{kind=link}
{kind=link}